Light Tissue Interactions
Recent advances in the understanding of light-tissue interactions, particularly with regard to selective photothermolysis and fractional photothermolysis have paved the way for more precise management of many cutaneous and superficial vascular disorders. Attention to managing the optical interface at the skin surface and progress beyond continuous laser beam outputs to pulsed lasers has mitigated adverse events allowing a wider therapeutic index.
Although there is sometimes limited clinical evidence base in this area, there is compelling theoretical and case based evidence for the efficacy of lasers which precisely target chromophores such as haemoglobin, water and melanin. No other modalities can treat vascular and pigmented lesions without damaging adjacent tissue. The wavelengths important to laser and other light based treatments in dermatology are: (UV; 200-400nm), (visible light; 400-760nm), (near infrared; 760-1400nm), (mid-infrared; 1.4-3μm) and (far-infrared; >3μm).
Lasers as light sources are unique because they can, depending on parameters, allow for exquisite control of tissue heating. Lasers can be highly effective in collimated, focussed or fractional delivery systems without having limitations of light beam attenuation. Filtered flash lamp (intense pulsed light) devices may also be useful in a broad sense but they lack beam directionality, spatial and temporal coherence and monochromaticity and are therefore inherently less accurate from a theoretical standpoint.
Narrowing the pulse width (energy delivery period) to very short time intervals allows for a photo-mechanical effect which enables treatment of pigmented lesions such as dermal melanocytosis and tattoos and lengthening the pulse width can target large structures like hair follicles so long as bulk cooling is adequate. The challenges of using lasers in skin of colour depends on an understanding of the ‘epidermal melanin paradox’ where increased melanin requires higher fluence treatments to achieve results with respect to other chromophores but as a radiation absorber melanin is prone to generating adverse reactions, so that a narrow therapeutic index exists.
Removing a chromophore eg pressure applied by diascopy to reduce oxyhaemaglobin will enable a pulsed dye laser to selectively treat superficial hyperpigmentation by eliminating the vascular component.
Together with dramatic increases in power delivery come potential risks due to high levels of oxidative stress associated with laser energy delivery. Significant short term skin injury can occur and although DNA damage leading to carcinogenesis is unlikely, careful physician monitoring is warranted, particularly with repeated laser treatments. Other clinical issues include laser targeting of melanin which can disguise atypical melanocytic lesions and can result in delayed diagnosis of melanoma.
Selective Photothermolysis
With the exception of water, skin chromophores are in relatively low concentration (of melanin, haemoglobin). 30 years ago Dr Rex Anderson described the concept of selective photothermolysis. ‘Extreme’ localised heating – enough to denature the target chromophore – was identified as reliant on (i) a wavelength that reaches and is preferentially absorbed by the intended target ‘structure’ (chromophore)
(ii) an exposure duration less than or equal to the time necessary for cooling of the target structure (thermal relaxation time), (iii) sufficient energy to damage the target (chromophore). These concepts allow for a relatively ‘large’ beam to ‘find’ its target.
Thermal Relaxation Time
This is the time taken for a target (chromophore) to cool to 50% of its peak temperature. Larger structures require relatively much more time to cool than smaller structures and this can be demonstrated mathematically. The thermal relaxation time (T) of a target structure will need to be longer than the time required to heat it up if it is to be treated (denatured). Size, shape and boundaries all affect this and
can be difficult to precisely define but T is normally equal to δ/gk where δ is the optimal penetration depth, k is the thermal diffusivity and g is a constant based on the geometry of the target.
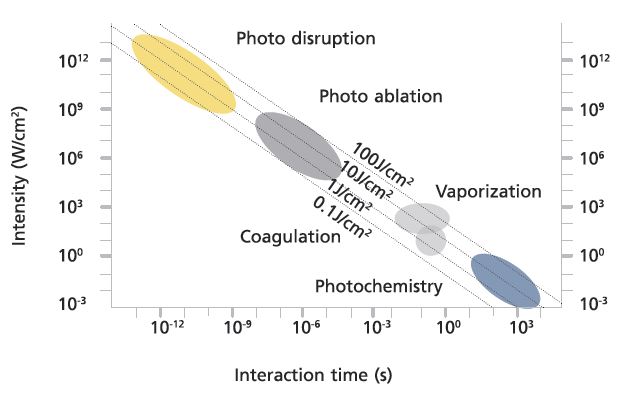
Tissue Reactions
- Photothermal: as temperature is raised, tissue coagulates. Thermal denaturation of proteins is temperature and time dependent. Photothermal processes depend on the type and degree of heating from coagulation to vapourisation. Milder heating results in breakage of hydrogen bonds and tissue alteration.
- Photomechanical (also referred to as photoacoustic due to the audible ‘snap’ during treatments): with very rapid heating there is insufficient time for pressure relaxation so that disassembly of tissue occurs with extensive microcracks. Inertially confined ablation occurs when there is high pressure at constant volume. With nanosecond pulsing energy is invested so quickly that there is no time for pressure release this is accentuated with pico-second devices.
- Photochemical: These reaction pathways are becoming increasingly important in dermatology. Singlet oxygen is created by photodynamic action after excitation of a photosensitiser by a specific wavelength of light. The ‘excited’ singlet oxygen state reacts with biological molecules ‘attacking’ plasma and cellular membranes. PDT is now a mainstay of treatment for certain superficial skin cancers.
- Protoporphyrin IX from aminolevulinic acid (ALA) is the most common endogenous photosensitiser in human tissue. Most photochemical reactions proceed most effectively with low power densities. Endogenous photochemistry generally occurs in the UVB range (less than 320nm) but ‘blue light’ treatments for acne depend on UVA (approx. 360nm) activation of endogenous porphyrins, most of the rest occur through the visible spectrum but photochemistry beyond 800nm is unlikely even with exogenous photosensitisers.
- Biostimulation/photomodulation: still a contentious issue but the concept is based on minor photochemical interactions. Generally low fluences from lasers of LED sources but no definite thermal effect. Visible light and new infrared LED sources might benefit wound healing and possibly facial skin texture and tone. More studies are required to look at these subtle effects on ‘subcellular’ processes and skin repair.
Fractional photothermolysis
This concept was devised in 2003 by Rex Anderson and Dieter Monstein and initially applied to near and mid infrared lasers. The laser creates multiple microthermal zones a fraction of a millimetre in diameter. These zones contain either coagulated tissue (non-ablative) or vapourised and adjacent necrotic tissue (ablative). The depth of penetration is controlled partly by wavelength (eg dermo-epidermal junction for the 1927nm non-ablative holmium laser) and partly by fluence (eg ablative CO2 laser 10600nm for infrared). Microthermal zone wounds are generally surrounded by viable tissue which speeds recovery and reduces side effects such as loss of skin colour.
Caution
- Skin surfaces must be properly cleaned of any reflective particles, absorbing chemicals (sunscreen), make up, creams which can alter the optical interface and any possible exogenous photosensitisers.
- All ingested medications (prescribed, OTC, herbal) must be recorded and checked. Most medication that photosensitises does so in the UV spectrum (eg tetracyclines) so these medications may be continued with most laser and light based treatments.
- Laser and light based treatments should be used with care when a patient is on systemic or topical retinoids. Although absorption spectra for both isotretinoin and tretinoin approaches zero at 450nm after peaking between 340nm and 350nm these molecules cause skin fragility through loss of epidermal cell adhesiveness and particular care should be taken with any resurfacing procedure which should be delayed for at least 3 months after completing retinoid treatment.
- Idiopathic photodermatoses such as solar urticaria may photosensitise in the visible spectrum and some autoimmune disorders such as light sensitive lupus, atopic dermatitis and chronic actinic dermatitis may be exacerbated by lasers and other light based treatments. A detailed history and examination are required to exclude these disorders.
- Pigmented photo-types should be prepared with a topical tyrosinase inhibitor such as 4% hydroquinone and strict sun avoidance/sunblocking should be practiced both before and after laser and light based treatment interventions.
The Electromagnetic Spectrum overlaid with absorption coeffiecient
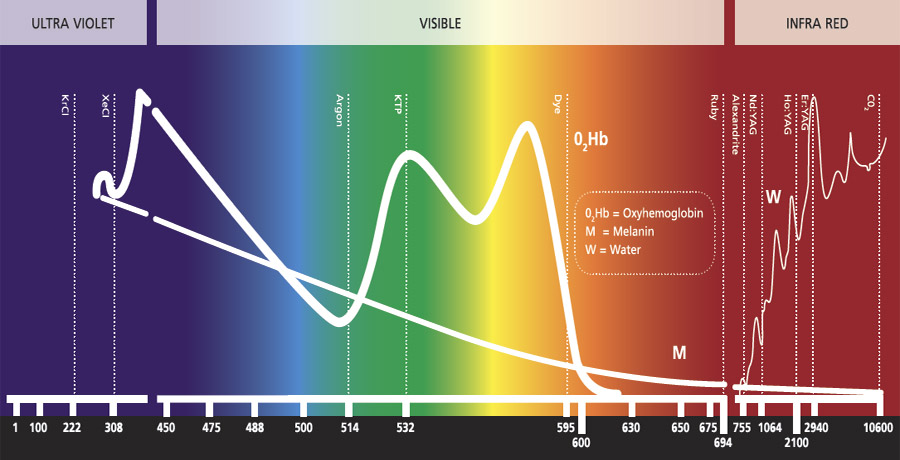
The Electromagnetic Spectrum
- Absorption coefficient for water declines less quickly than for O2Hb
- H2O concentration high in tissue is critical at infrared wave lengths
- Near IR window (optical or therapeutic window) in biological tissue
- Light scattering is dominant and leads to rapid diffusion of propagating light